Healthcare Team, Aki Kawamura
You get facts from surveys, and to make use of those facts, you would need to find out the "whys" — the causal factors behind it. Reaching the "why" can be done through interviews or by open-ended questions in surveys, but we often hear from our clients that it needs a lot of time and skills to analyze.
In this article, we will introduce how we derived the “why” from the results of our survey on diabetes drugs. Our proprietary analytic tool, Key Explorer, enabled us an easy and quick process to come out with actionable measures by drawing personas from a deep dive into each target.
Doctor’s Choice of Oral Hypoglycemic Drug
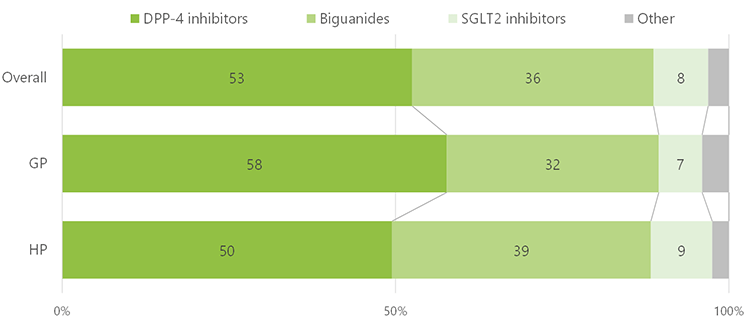
Today, there are 8 types of oral hypoglycemic drugs available in Japan. DPP-4 inhibitors were the most frequently chosen (53%). Followed by biguanides at 36%. With these two drugs combined, the adoption rate reaches nearly 90%. The next common was SGLT2 inhibitors at 8%. Other remaining 5 types of drugs were rarely picked. Dividing the doctors into groups of general practitioners (GP) and hospitals (HP), DPP-4 inhibitors were slightly more chosen by GP.
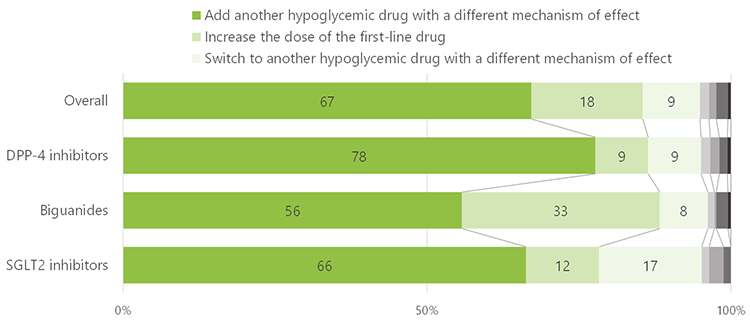
When the event of the ineffectiveness of first-line drugs, “add another hypoglycemic drug with a different mechanism of effect” was the top subsequent treatment at 67%. Other alternatives were “increase the dose of the first-line drug” and “switch to another hypoglycemic drug with a different mechanism of effect”. Comparing the top 3 doctors’ choice of drugs, those who chose DPP-4 showed 10 points higher than overall in selecting “switch to another hypoglycemic drug with a different mechanism of effect”, while those who selected “increase the dose of first-line drug” was 10 points lower. For biguanides, “increase the dose of the first-line drug” was 15 points higher than the overall, while the number of doctors who “add another hypoglycemic drug with a different mechanism of effect” decreases. In the case of doctors who chose SGLT2, “add another hypoglycemic drug with a different mechanism of effect” increases.
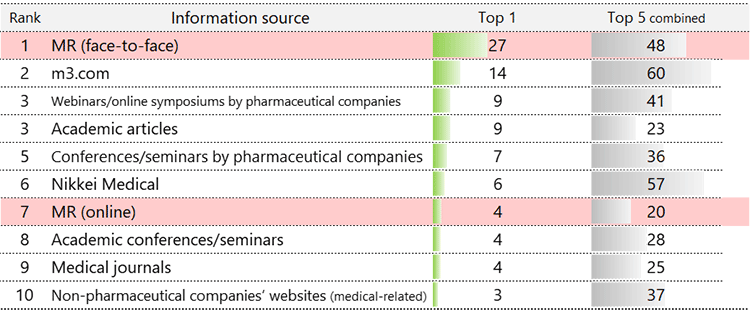
The most referenced source of information on diabetes treatment is “face-to-face communication with MRs (Medical Representatives)”. Combining all 1st to 5th most referenced source, M3 (m3.com) and Nikkei Medical are the top 2 at around 60%, but the combined total of MRs (face-to-face and online communication) reach 70%, making them the highest. With the COVID-19 pandemic, we have heard numeral discussions elsewhere on the positioning of MRs as opposed to digital, or the value of them, but this indicates that MRs are still an important source of information for doctors.
Doctor Types and How to Communicate with Them
So, what kind of information do doctors value, and how should it be delivered? Through MRs or other channels?
In a short answer, you will need to clarify the target and communicate accordingly depending on each characteristic.
We classified doctors into 3 types according to their choice of first-line drug. The characteristics of each type are compared in the following 3 aspects: (a) profile, (b) attitudes and behaviors toward medical care, and (c) sources of information about treatment.
First-choice: DPP-4
A veteran internist of 60s+, highly interested in the latest developments.
- Work in a clinic or physician’s office with no beds.
- Do not consider health care economics for their treatment decisions.
*Maybe rooted in their work in the clinic.
- Highly interested in drug therapy trends and are the type that actively gathers information, even knowing it to be as an advertisement.
- Information sources are MRs and non-pharmaceutical companies’ websites.
First-choice: Biguanides
Young, conservative, specialists in their 30s.
*Biguanides are looked at as a good-old classic medicine.
- Doctors in their 30s who work in a large national/public hospital with more than 400 beds.
- A careful doctor who makes treatment decisions by considering the health care economics and seeks full consensus on the latest treatments.
- Is reluctant to contact MRs.
- Has high expectations toward “digital health”.
- Speaks at academic conferences, seminars, and webinars.
- Books, academic articles, conference publications, and medical journals, are their information sources.
First-choice: SGLT2
Early majority, eager for knowing the details.
*Early majority is the segment that adopts new things faster than average, among the 5 tiers of the “Diffusion of innovations” theory.
- No characteristics were found based on individual profiles such as age or specialty.
- Work in private hospitals with 20-99 beds.
- Looks out for new things and trends but go one step further — adopting drugs that are known to be more effective and the latest therapies, much faster than others.
- MRs (face-to-face) is their source of information.
- Proactively communicate with MS (Marketing Specialist).
*Considering the MRs to be their information source, they would meet with MS when they are visited, rather than gathering information from MS by themselves.
We looked at the reasons for choosing that drug by each doctor type.
DPP-4 first-choice doctors' reasons are “safe with fewer side effects and hypoglycemic risk,” “easy to use for the elderly and people with renal impairments,” and “effective under just 1-dose-a-day”. If the effect is inadequate, an addition of a second-line drug is mentioned, while biguanides or SGLT2 are chosen in such cases.
Biguanide first-choice doctors' reasons for choosing are “recommended by domestic/European/US guidelines” and “drug price is inexpensive”. In the case of insufficiency of the first-line drug, they tend to “increase the dose of the first-line drug”. Despite the number of doctors who “add another hypoglycemic drug with a different mechanism of effect” being higher, their tendency to increase the dose is unique compared to other types. DPP-4 is cited as their second-line drug because it is “safe with fewer side effects” and “(aligned with) guidelines”.
SGLT2 first-choice doctors' reasons are more specific: “can be used in patients with impaired function,” “effective in reducing cardiovascular events,” “expectation on renoprotective effect,” and “prevents complications”. In the case of ineffectiveness, they would switch to another drug, and DPP-4 would be their next choice.
From the above doctor types, we can think of the following communication approaches.
DPP-4 first-choice doctors are relatively engaging digitally for their source of information. Not on pharmaceutical company websites but looking for information on online media. They also expect face-to-face meetings with MRs. To actively release on websites other than the corporate website, advertising in digital media may be an option to consider, too.
Biguanide first-choice doctors would be effective to provide data to authoritative media. Should watch out not to induce negative reactions by MRs and other human-based interactions. Provide information focused on guidelines and trends in Europe/US for building more confidence and insert information in which they are highly interested, such as digital health.
SGLT2 first-choice doctors are not only interested in the latest developments, but they also adopt the drug. To provide the latest academic trends by engaging through MRs is similar to DPP-4 first-choice doctors, however, the key for this type would be to explain the safety and efficacy in more detail. Utilizing the MS may be another aspect to consider.
Personas (doctor types) by Key Explorer
Once you understand the personas of each target, it will be easy to plan actions connected to their characteristics. Usually, checking cross-tabulations of survey data from various breakdowns would be necessary before creating those personas. Which will take much time to look through the data and requires certain experience in data analysis.
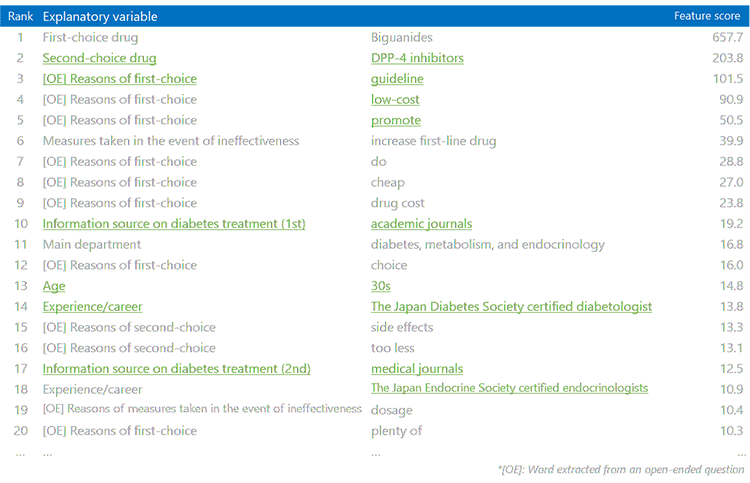
Nikkei Research's proprietary analytic tool, Key Explorer, enables one-stop analysis across all data, from numerical values to texts. It produces a ranking based on the statistical strength of characteristics, automatically. That will allow you to observe results in a short time without missing out on the important insights.
Example of the feature score ranking (from the survey on diabetes drugs)
Survey Methodology
Conducted between March 8-9, 2022. Physicians of general internal medicine and diabetes, metabolism, and endocrinology who are registered to Nikkei Medical Online were randomly selected to participate in the survey. Collected responses from a total of 1,010 physicians. The survey asked questions regarding their profiles, treatment status, prescribing status and reasons for prescribing, information sources and interactions, and communication with pharmaceutical companies. The length of the survey was averaged at approx. 30 min.
*Please note that results are from a survey using a registered panel and may differ from medical records data.

Key Explorer is widely used for CX, innovation, and finding insights. While tools do not solve everything, good planning and design of the survey/questionnaire are also important for getting the best outcomes.
Nikkei Research will make sure you onboard and provide full support throughout your projects.
Please contact us if you are interested to know more.

